There are three stages of the adult acquired flatfoot:
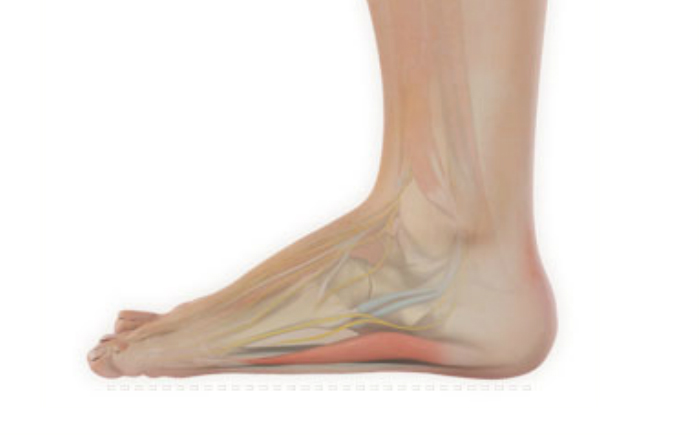
Stage I: Inflammation and swelling of the posterior tibial tendon around the inside of the ankle.
Stage II: Visible deformity comparing one foot to the other, as the symptomatic foot becomes flatter and more deformed. The deformity is movable and correctable in this stage.
Stage III: The foot progresses to a rigid, non-movable flat foot deformity that is painful, primarily on the outside of the ankle
Diagnosis:
The adult acquired flatfoot, secondary to posterior tibial tendon dysfunction, is diagnosed in a number of ways with no single test proven to be totally reliable.
The most accurate diagnosis is made by a skilled clinician utilizing observation and hands on evaluation of the foot and ankle. Observation of the foot in a walking examination is most reliable. The affected foot appears more pronated and deformed compared to the unaffected foot. Muscle testing will show a strength deficit. An easy test to perform in the office is the single foot raise.
A patient is asked to step with full body weight on the symptomatic foot, keeping the unaffected foot off the ground. The patient is then instructed to “raise up on the tip toes” of the affected foot. If the posterior tibial tendon has been attenuated or ruptured, the patient will be unable to lift the heel off the floor and rise onto the toes. In less severe cases, the patient will be able to rise on the toes, but the heel will not be noted to invert as it normally does when we rise onto the toes.
X-rays can be helpful but are not diagnostic of the adult acquired flatfoot. Both feet – the symptomatic and asymptomatic – will demonstrate a flatfoot deformity on x-ray. Careful observation may show a greater severity of deformity on the affected side.
Magnetic Resonance Imaging (MRI) can show tendon injury and inflammation but cannot be relied on with 100% accuracy and confidence. The technique and skill of the radiologist in properly positioning the foot with the MRI beam are critical in demonstrating the sometimes obscure findings of tendon injury around the ankle. Magnetic Resonance Imaging (MRI) is expensive and is not necessary in most cases to diagnose posterior tibial tendon injury.Ultrasound has also been used in some cases to diagnose tendon injury, but this test again is usually not required to make the initial diagnosis.
Treatment:
The adult acquired flatfoot is best treated early. There is no recommended home treatment other than the general avoidance of prolonged weightbearing in non-supportive footwear until the patient can be seen in the office of the foot and ankle specialist.
In Stage I, the inflammation and tendon injury will respond to rest, protected ambulation in a cast, as well as anti-inflammatory therapy. Follow-up treatment with custom-molded foot orthoses and properly designed athletic or orthopedic footwear are critical to maintain stability of the foot and ankle after initial symptoms have been calmed.
Once the tendon has been stretched, the foot will become deformed and visibly rolled into a pronated position at the ankle. Non-surgical treatment has a significantly lower chance of success. Total immobilization in a cast or Camwalker may calm down symptoms and arrest progression of the deformity in a smaller percentage of patients. Usually, long-term use of a brace known as an ankle foot orthosis is required to stop progression of the deformity without surgery.
A new ankle foot orthosis known as the Richie Brace, is available from a number of podiatric labs (www.Richiebrace.com), has proven to show significant success in treating Stage II posterior tibial dysfunction and the adult acquired flatfoot. This is a sport-style brace connected to a custom corrected foot orthotic device that fits well into most forms of lace-up footwear, including athletic shoes. The brace is light weight and far more cosmetically appealing than the traditional ankle foot orthosis previously prescribed.
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions. (See surgical correction of adult acquired flatfoot)
Patients with adult acquired flatfoot are advised to discuss thoroughly the benefits vs. risks of all surgical options. Most procedures have long-term recovery mandating that the correct procedure be utilized to give the best long-term benefit. Most flatfoot surgical procedures require six to twelve weeks of cast immobilization. Joint fusion procedures require eight weeks of non-weightbearing on the operated foot – meaning you will be on crutches for two months.
The bottom line is: Make sure all of your non-surgical options have been covered before considering surgery. Your primary goals with any treatment are to eliminate pain and improve mobility. In many cases, with the properly designed foot orthosis or ankle brace, these goals can be achieved without surgical intervention.